Omega-3s are a family of essential polyunsaturated fatty acids that play an important role in the body and may provide a number of health benefits. Since the body cannot produce them on its own they are obtained through diet. Their consumption is associated with a lower risk of cardiovascular diseases, reduction of arterial hypertension, normalization of triglyceride and cholesterol levels and anti-inflammatory properties that may have an effect on the symptoms of rheumatoid arthritis.
The three most important types of Omega-3 unsaturated fatty acids are ALA (alpha-linolenic acid), DHA (docosahexaenoic acid) and EPA (eicosapentaenoic acid). ALA is obtained mainly from plant sources (flaxseed, rapeseed, walnut, chia, etc.), while DHA and EPA are found mostly in seafood such as salmon, mackerel, trout, mussels, shrimp, crab and also in various algae.(1)
ALA is a dietary precursor in the body that is transformed into EPA and DHA after consumption. Unfortunately, ALA has no high biological activity and no significant contribution to health unless it undergoes conversion to EPA or DHA. The problem is that the effectiveness of the transformation, which occurs mainly in the liver, is very limited with reported levels below 15%. Therefore, consuming EPA and DHA directly from foods and/or supplements is the only practical way to increase beneficial Omega-3 fatty acid levels in the body.
High levels of Omega-6 fatty acids are found in commonly consumed foods such as animal fats, vegetable oils (sunflower, corn), various nuts and seeds and some grains. Omega-6 fatty acid most commonly obtained through diet is linoleic acid, which the body converts to arachidonic acid (AA).
Eicosanoids are signaling molecules (prostaglandins, thromboxanes, leukotrienes, lipoxins, etc.) that control inflammation signals in the body via autocrine, paracrine and endocrine pathways. They are produced by the enzymatic or nonenzymatic oxidation of arachidonic acid (AA), Omega-3 (EPA, DHA), etc. (Figure 1).(2)
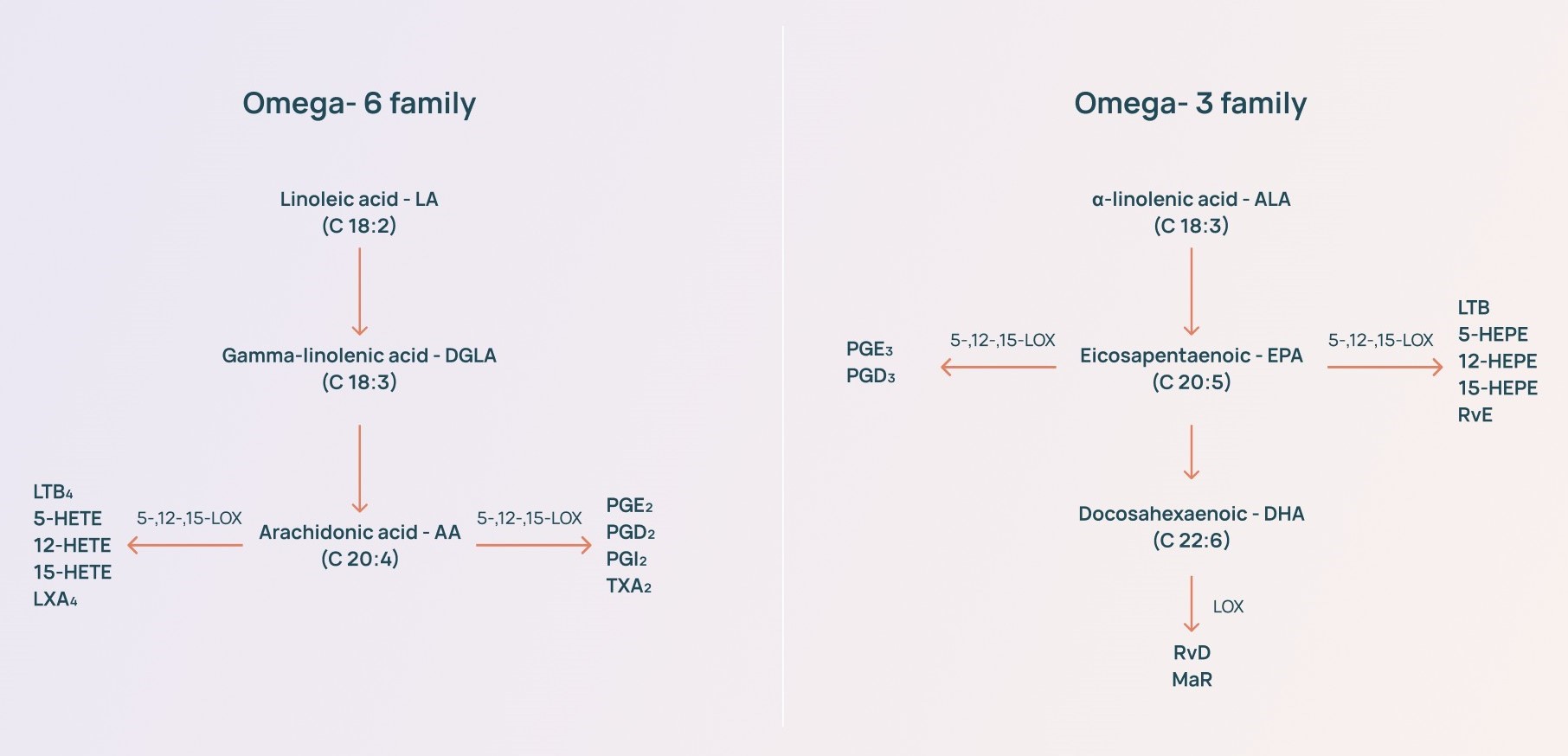
Eicosanoids produced by Omega-6 fatty acids are more powerful mediators of inflammation, vasoconstriction and platelet aggregation compared to those derived from Omega-3 fatty acids.
Since both fatty acid classes compete for the same enzymes, EPA and DHA compete with arachidonic acid for eicosanoid synthesis. Thus, higher concentrations of EPA and DHA than arachidonic acid direct the eicosanoid balance toward a lower inflammatory potential.(3)
Omega-6/Omega-3 ratio
The optimal healthy balance of Omega-6 to Omega-3 consumption is approximately 4:1. The Western dietary pattern is largely associated with intake of high amounts of Omega-6 fatty acids relative to Omega-3 fatty acids in the range of 15 to 20:1. The high Omega-6/Omega-3 ratio is associated with the pathogenesis of many diseases, including cardiovascular, oncological, inflammatory and autoimmune diseases.(4)
The combination of Omega-3 fatty acids with Vitamin D and light physical activity has shown preventive qualities with reduction in cancer incidence in the elderly.(5)
Data from 7 clinical studies of cachectic patients with lung cancer show a statistically significant contribution of Omega-3 fatty acid supplementation versus placebo in reduction of cachexia and improvement of the quality of life (QoL).(6) Other studies demonstrate that Omega-3 fatty acid supplementation is associated with reduction of neurotoxicity induced by CT (Oxaliplatin) (7), reduction of inflammation and lowered inflammatory serum markers (8), and synergistic potential in combination with standard antitumor treatments.(9)
Dose, side effects and cross-reactions
The recommended daily intake of Omega-3 fatty acids for adults over 18 years old is 1.1 g a day for women and 1.6 g a day for men.(10) Continued intake of doses higher than 10 g/day may result in complaints of heartburn, diarrhea and bleeding.
Concomitant intake of high doses of Omega-3 fatty acids with antihypertensives, Cyclosporine, Sirolimus and Tacrolimus (Prograf) may potentiate their effects and side reactions.(11)
In some more sensitive people intake of high doses exceeding 1 g/d of Omega-3 fatty acids in the fasting state may cause gastrointestinal discomfort and/or a single liquid bowel movement without an increase in frequency.
If symptoms persist reduce Omega-3 fatty acid intake according to individual sensitivity.






